
InterRAI
Overview of InterRAI
The InterRAI is a comprehensive person-centered review of the participant’s health and functioning, in order to properly assess their needs for services
- InterRAI is completed in Function Portal. Once you have a visit scheduled in Function Portal you will be able to document the visit note (ie. see alert on the right hand side of the screen in FP). Once the visit note is submitted you will then see an alert to be able to document the InterRAI.
- All of the questions in the InterRAI must be answered.
- NEVER guess or assume answers. If you are unsure about which answer to select, ask the participant more specific questions and then select the appropriate response.
- Start with broad questions about the section
- Get more specific when needed based on the participant’s answers
- Be consistent
- There is a lot of overlap between sections of the InterRAI, and between other documents during your comprehensive needs assessment. Your answers need to match between the InterRAI, PCSP, HEDIS, and the visit session.
- There are several different sections to the InterRAI session, below are some examples of information that is covered in the assessment
- Demographic and General Information about the Participant
- Participant’s Health and Functioning (ADL/IADL’s)
- Informal supports and Formal Care
- SPG Tool: This tool is automatically populated once you have completed all prior sections.
Helpful Tips & Examples
Identification Information
Demographic and other general information about the participant. Much of this information can be found on the participant’s Info tab of Function Portal (this information is to be verified with the participant when doing the assessment and the information in the InterRAI and in the Info Tab must match)
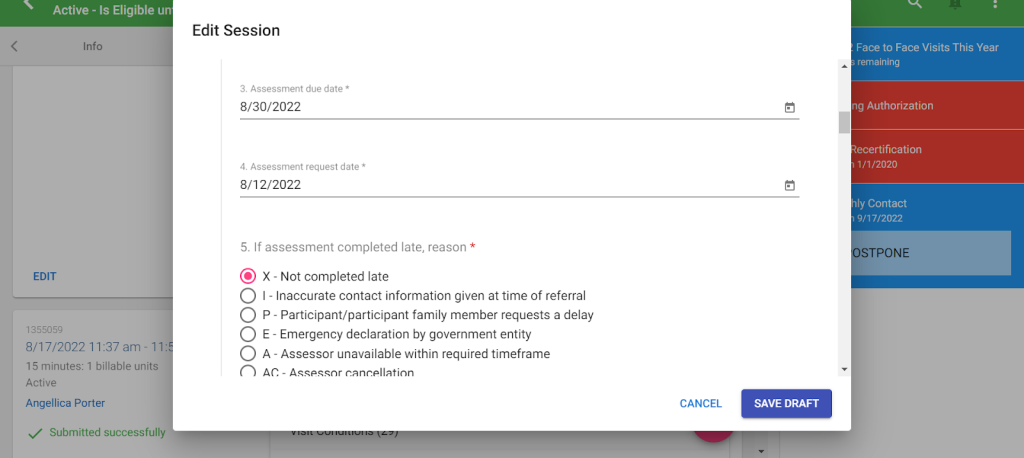
Assessment Dates
The assessment due date is either indicated in Function portal in the alerts on the right hand side of the screen (for Annual visits), must be within 5 days of the receipt of the participant (NPO visits) or it is within 14 days of the discharge from the hospital or the request for a visit from the participant (for Change Events). You MUST ensure the dates are correct and then select a corresponding reason.
Example:
Marital Status
- If the participant is listed as “Single” in Function Portal, double check if they have been married in the past (then change Function Portal if necessary)
- Partner/Significant Other are the same and include those the participant is romantically close to, without being legally married
- They may even refer to each other as spouses even if they aren’t actually married
Payment Sources
Select Yes or No based on if the participant uses the following payment sources for Services. Information from this section MUST match the Info Tab in Function Portal.
Medicaid – All participants use Medicaid. Therefore the answer should be 1-Yes
Medicare – Answer will depend whether or not the participant has Medicare (check the Eligibilities tab in FP and verify with the participant during the visit
Medicare with Medicaid co-payment – Selected “yes” if the client has both Medicare and Medicaid.
Example:

Reason for Assessment
Select the answer that applies to the type of visit you are completing, it must match
- New Participant Orientation (NPO) visits; answer is 1 – First Assessment
- Annual Visit; answer is 2 – Routine Assessment
- Change Event visit; answer is 3 – Return Assessment or 4 – Significant Change in Status Reassessment depending on why you are completing the visit.
- If you are doing the visit because you need to address a participant requesting a change in services (with no change in their health), or to follow up on a critical incident that did not actually change the participant’s health then select (3 – Return Assessment)
- If you are following up because there was a change in their health or caregiver, select (4 – Significant Change)
Example:

Person’s Expressed Goals of Care
- State the participant’s goal in having/receiving services and care in a full sentence.
- Then, state the goal again in just a couple of words below.
Example:

Primary Language/Race & Ethnicity
State the participant’s actual primary language, Not just the language they are speaking to you in. For race, ask what the client identifies as, DO NOT assume. You need to verify this with the participant during the visit.
Participant’s health and functioning
Cognition
This section is made up of questions regarding the participant’s cognitive ability to make decisions, maintain memory, and their awareness. If you indicate on the InterRAI that the participant has any issues with Cognition, then the PCSP must indicate the same information, as well as be consistent with the visit note and HEDIS. Higher scores mean more significantly impacted cognitive performance.
Memory Quiz – to test a participant’s short-term memory give them the following quiz. This is not a diagnostic tool. It just helps pave the way for better conversation on the topic if necessary.
- Ask the participant to remember 3 random objects
- Move on with more of the assessment, then in 5 min or so ask the participant if they remember the objects.
- If they forgot 2 or all 3 objects, then they may have a short-term memory problem.
- If they forgot only 1 object, then their short-term memory may be ok (or have more of a conversation with them about it)
- Ask the participant about the 3 objects again at the end of the assessment to test their Long-Term Memory.
Mood and Behavior
Discussion about the participant’s recent mental health and behavior.
Note: This section is specifically asking about indicators of the last 3 days.
Locomotion and Walking
Timed 4-meter walk
- Have the participant walk a straight, unobstructed path, across a room (about 13 feet) and time them. Your answer is how many seconds it takes for them to do so.
- If the participant needs to stop for any reason, stop and put answer 77 – Stopped before test complete
- If the participant refuses to do the walk, or you refuse to for any reason, put 88 – Refused to do the test
- If the participant is not capable of walking in any way, put answer 99 – Not tested
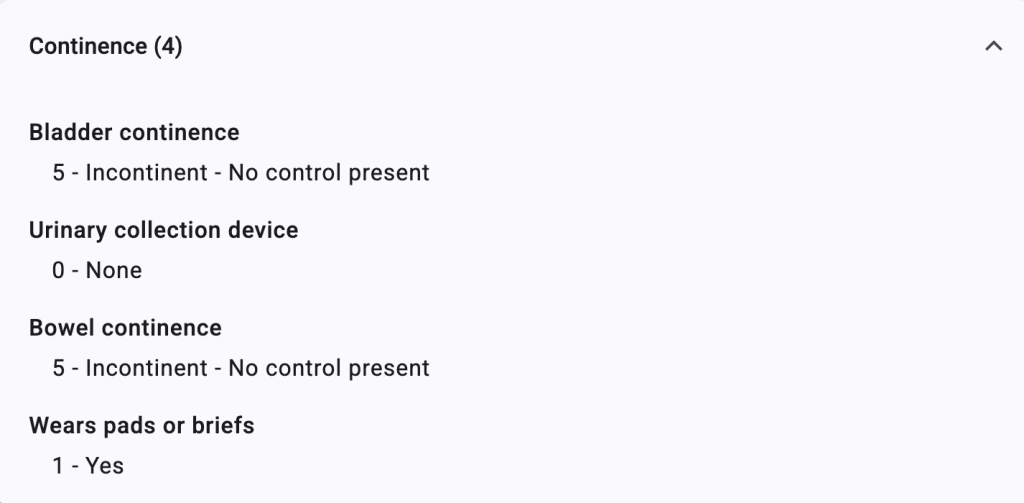
Continence
Section 33 of InterRai: Bladder/Bowel continence reflects a person’s pattern of urinary/bowel control, considering any support strategies such as:
- Scheduled toileting
- Continence training programs
- Prompted voiding or reminders
- Use of urinary devices
- Use of incontinence supplies
⚠️ Important:
- Bladder/bowel continence is not the same as toileting ability. A person can require assistance with toileting and still be considered continent.
- Any urine/bowel leakage (dribbling, bowel accidents or wetting) is considered incontinence.
If the participant requires or is requesting incontinence supplies, this section should indicate the need for supplies if the participant is requesting them at the time of the visit.
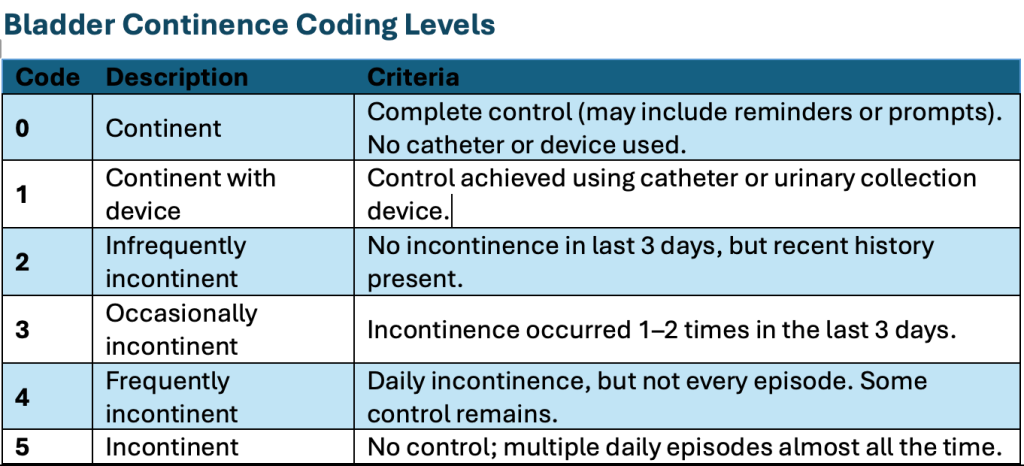

Key Coding Tips
- Focus on pattern over the last 3 days.
- Consider all interventions or supports in place.
- Evaluate frequency, not just presence, of incontinence.
Pads or Briefs Worn (iH4)
Definition
This item identifies whether the person uses:
- Absorbent briefs (e.g., adult diapers)
- Pads (worn or placed on surfaces like beds/chairs)
- Includes both disposable and reusable products.
Select yes for pads/briefs if:
- Due to bladder/bowel incontinence
- For protection from urinary leakage/bowel
Select no for pads/briefs if:
- Used for non-incontinence reasons
- Used routinely when the person is never incontinent- Example: A woman wears pads due to menstrual cycle flow/bleeding but is fully continent.
Critical Rule
✅ Only answer iH4 based on information gathered in Section H (continence assessment).
❌ Do not consider unrelated use of pads or briefs.
Documentation Best Practices
- Always document in toilet use ADL justification (example below):
- Frequency of incontinence episodes
- Timing (day/night patterns)
- Use of devices or interventions
- Ensure consistency between:
- iH1 (continence level)
- iH4 (pad/brief use)
- Ensure consistency in other assessment documents including visit note and PCSP

Diagnosis and Problems
Documentation of the participant’s diagnoses. Pay close attention to the key/code and be sure to document any diagnoses the participant has.
- 0 – Not present – If the participant does not have the diagnosis
- 1 – Primary diagnosis – the primary reason why the participant requires care (This option should not be used in Sections 34-38 of the InterRai because you will select a primary diagnosis in Section 39)
- 2 – Diagnosis present, receiving active treatment – a diagnosis, besides the primary, for which the participant is currently being treated for
- 3 – Diagnosis present, monitored but no active treatment – a diagnosis, besides the primary, for which the participant is NOT receiving treatment for.
Other Disease Diagnosis – You will check off the primary diagnosis which is the primary reason why the participant requires care. Additionally, you will select up to 6 other diagnoses that affect daily functioning.
Example:

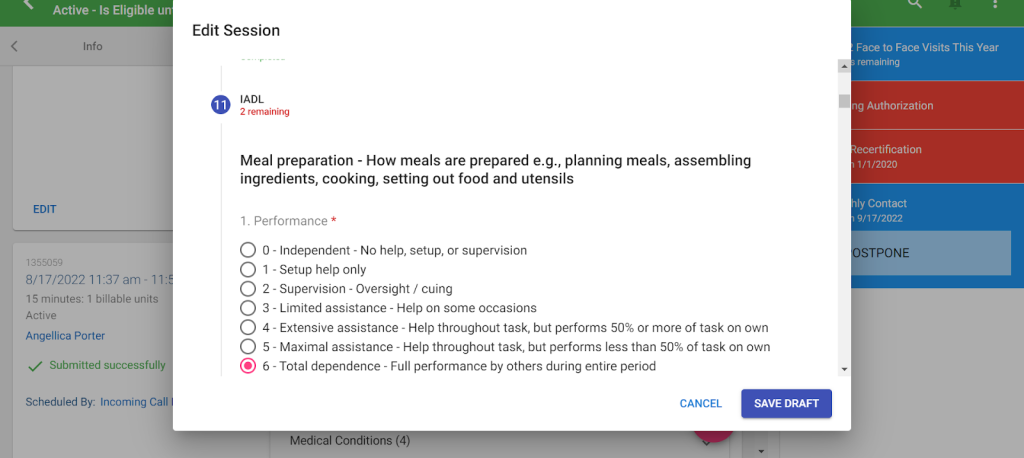
IADL’s (Instrumental Activities of Daily Living)
These are activities that are done daily or regularly to take care of the participant and their home. IADL’s require complex planning and thinking to complete. Discussion of how each activity is being performed currently should take place with the participant and their Person Centered Team, during the visit. Then select the option that most closely aligns.
Example:
Discussion of what the participant’s capacity is to perform that same activity and what days they require assistance with this activity each week.
Please note: When selecting days of the week the participant requires assistance, this refers to ONLY days when formal assistance (ie. PAS hours) would be needed
Example:

Discussion of the need for additional support to what is currently in place (either formally or informally) should take place. Additionally, rationale for all services must be included and this includes providing information on the following:
-whether the participant receives informal support or not for the specific task
-what services are currently in place and what other services were offered (ie. shower chair was offered and accepted OR shower chair was offered and declined)
-information about diagnosis or needs that are relevant to this activity
-clear statement on what the service that is put into place will be doing to assist (ie. HHA assists with meal preparation for dinner).
Example:

ADL’s
These are basic self-care activities that are done daily or regularly to take care of the participant and their home. Discussion of self performance of each task should take place with the participant and their Person Centered Team, during the visit. Then select the option that most closely aligns.
Please note: When selecting days of the week the participant requires assistance, this refers to ONLY days when formal assistance (ie. PAS hours) would be needed
Example:

The days each week that the participant will need formal assistance should be discussed and corresponding days should be selected. Additional hours can be added, but only with justification.
Example:

Discussion of the need for additional support to what is currently in place (either formally or informally) should take place. Additionally, rationale for all services must be included and this includes providing information on the following:
-Whether the participant receives informal support or not for the specific task
-what services are currently in place and what other services were offered (ie. shower chair was offered and accepted OR shower chair was offered and declined)
-information about diagnosis or needs that are relevant to this activity
-clear statement on what the service that is put into place will be doing to assist (ie. HHA assists with meal preparation for dinner).
Example:

Discharge
If there was no hospital or NF stay then for “Last day of stay” you will type “12/31/2099”
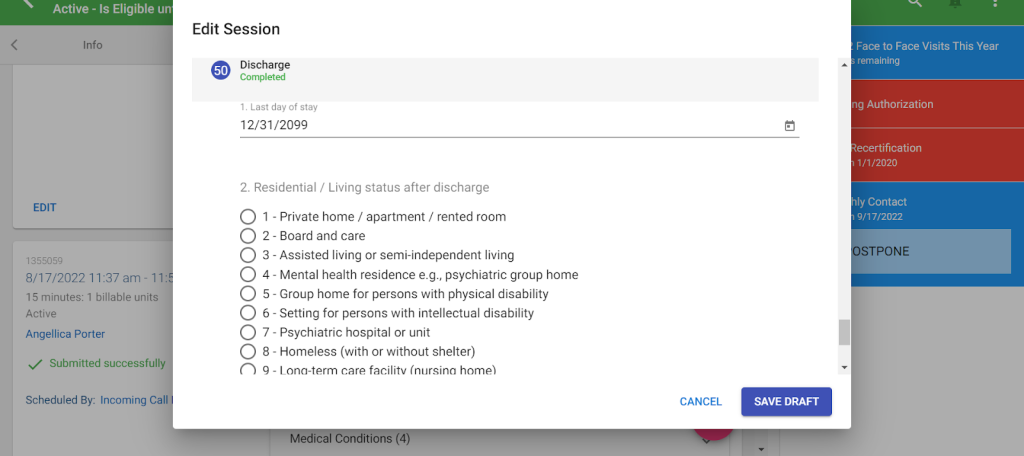
If there was no hospital or NF stay then for “residential/living status after discharge”, select “other”

Tips for IADL’s/ADL’s:
IADLs – Instrumental Activities of Daily Living
Self-care tasks that are necessary to live independently in the world. If these activities are not performed, it would result in a risk to a participant’s ability to live independently.
IADL Tasks
| Task | Details |
| Meal Preparation | -How meals are prepared-Includes: Planning/Deciding what food will be made for each meal, Preparing ingredients, Actually cooking and using appliances, setting up the dishes and utensils |
| Ordinary Housework | – How ordinary work around the house is performed – Includes: doing dishes, tidying up, dusting, vacuuming, making the bed, laundry, cleaning the bathroom. |
| Managing Finances | – How bills are paid, checkbook is balanced, household expenses are budgeted, credit card is monitored |
| Medication Management | – Includes: reminders to take medications, opening bottles, taking correct drug dosages, giving injections, and applying ointments |
| Phone Use | – How telephone calls are made or received Includes: assistance using assistive devices with phone use |
| Stairs | – How going up and down full flight of stairs is managed |
| Shopping | – How shopping is performed for food and household items – Includes: knowing what items are needed, choosing items, grabbing items and putting them in a cart, pushing a cart, paying money, bagging and carrying items. – EXCLUDE TRANSPORTATION |
| Transportation | – How participant travels by public transportation or drives themselves- Includes: navigating the public transit system, paying money for fares, getting in and out of the house and vehicles. |
IADL scoring
IADLs are scored the same based on Performance and Capacity.
- Performance – the summation of actual performance of the task for the past 3 days.
- Capacity – the presumed capability of the participant to complete the task.
- This is gathered from conversation with the participant and caregivers as well as speculation of the participant. If you feel the participant is more or less capable of completing a task than was given in the performance, then the capacity score should reflect it.
Scores
| Score | Description | Example |
| 0 | Independent No help, setup, or supervision Meaning the participant does not need any assistance at all with the task. | Ex. The participant states they don’t need any assistance making or receiving calls |
| 1 | Setup Help Only The participant needs someone to set up all the necessary tools to complete the task, but then they can do the task without assistance. | Ex. The participant needs her daughter to get all bills and finances together, but once it is together, the participant does the work themselves. |
| 2 | Supervision The participant needs someone to watch over them and make sure they do the task correctly, but still do all parts of the task themselves. | Ex. The participant needs their caregiver to remind the participant and make sure they take their medications, but they organize and take them by themselves. |
| 3 | Limited Assistance The participant can do the task themselves sometimes, but other times they need assistance. | Ex. The participant reports that they need weight bearing assistance with stairs only when their pain is unbearable but when pain is controlled, they are able to ambulate on stairs independently. |
| 4 | Extensive Assistance The participant needs assistance every time they complete the task, but are able to do more than half of said task on their own. | Ex. The participant goes shopping with a caregiver or informal support every time they need to go shopping, but they will push the cart, choose items, and pay for it themselves. The caregiver will lift items selected, place them into the cart and carry heavy bags |
| 5 | Maximal Assistance The participant needs assistance every time they complete the tasks and they do less than 50% of the task themselves | Ex. The participant needs assistance for housework, they are able to use a duster on all reachable surfaces, but the caregiver or informal support does the high surfaces, vacuuming, mopping/sweeping, laundry, etc. |
| 6 | Total Dependence The participant has absolutely no involvement in the task. If it weren’t for the caregivers it would not be done. | Ex. The participant needs someone to take them upstairs, they cannot take any steps themselves and if no one is around they don’t go up or down stairs. |
| 8 | Activity did not occur In the past 3 days the task was not done at all. This is NOT used when scoring capacity (because capacity is based on some speculation.) | Ex. The participant has not left the house in the past 3 days and therefore did not need transportation anywhere. |
ADLs – Activities of Daily Living
Daily tasks that are necessary to remain healthy. If these are not performed it would result in immediate risk to the participant’s health or safety.
ADL – Tasks
| Task | Details |
| Bathing | – How a full bath/shower is taken – Includes: Transferring in and out of the tub/shower and how each part of the body is washed |
| Personal Hygiene | – How personal hygiene tasks are managed/completed. – Includes: washing face, brushing teeth, washing hands, putting on makeup, shaving, etc |
| Dressing Upper Body | – How dressing/undressing above the waist is managed. – Includes: underwear and outerwear, fastening buttons, zippers, prostheses, orthotics, etc. |
| Dressing Lower Body | – How dressing/undressing from the waist down is managed. – Includes: underwear and outerwear, fastening buttons, zippers, prostheses, orthotics, etc. |
| Walking | – How ambulation from one point to another is managed. – Includes: getting in and out of a bed, chair, or sofa, walking with or without assistive devices from one point to another while on the same floor. -Note: you should say “this activity did not occur” if the participant strictly uses a wheelchair or is bed bound |
| Locomotion | – How the use of durable medical equipment for ambulation (including wheelchairs) – Includes: if reminders or hands on help is provided to the participant to use assistive devices. – Note: the only time you should say “this activity did not occur” is if the participant does not use any assistive devices or if the participant is bed bound. |
| Transfer Toilet | – How they move on and off the toilet or commode. – Note: This is just for getting on and off of a toilet or commode. If the ptp is completely incontinent and does not use a toilet or commode, then this activity does not occur. |
| Toilet Use | – How using the toilet/commode/incontinence supplies is managed. – Includes: wiping themselves after going to the bathroom, either the toilet/commode or incontinence supplies, changing pads/diapers or other incontinence supplies, managing ostomy and/or catheters, readjusting clothes after going to the bathroom. |
| Bed Mobility | – How movement in bed is managed. – Includes: assistance moving from a lying position to sitting upright and vice versa, turning from side to side in the bed, changing positions in bed. |
| Eating | – How eating and drinking is managed- Includes: intake of food by other means such as tube feeding. – Note: It is NOT about modification of food, that is included in Meal Prep |
ADL scoring
ADLs are only scored on performance of the last 3 days
- If every single time the activity occurred was at the same level, then score the task at that level.
- Ex. If the participant says every time they take a bath/shower they just needed someone nearby to supervise, then you should give them the score for “Supervision”
- If any episode in the past 3 days was a 6, and others were less dependent, then score it at 5.
- Ex. If the participant says “Yesterday I was not able to move around in my bed at all, but today and most other days I can at least readjust myself” then you should give them a score of 5
- Otherwise, if the participant says their ability to complete tasks has fluctuated a lot in the last 3 days, focus on the 3 most DEPENDENT episodes.
- Ex. In the past 3 days the participant has completed personal hygiene 3 times. For two out of the three times, they needed maximal weight bearing assistance (5),. For one out of the three times, the participant needed extensive weight bearing assistance (4). Score as a 5 because the majority of tasks required maximal.
ADLs Scores
| Score | Description | Example |
| 0 | Independent No physical assistance, setup, or supervision in any episode The participant does not need any setup help, supervision, or assistance at any point throughout the task. | Ex. The participant states they are able to feed themselves after all food is prepared and placed in front of them. |
| 1 | Independent, setup help only Article or device provided or placed within reach, no physical assistance or supervision in any episode. The participant needs someone to setup whatever is needed for the task, but then completes the task on their own. | Ex. The participant needs someone to place their hairbrush and toothbrush in reach and then is able to complete the task themselves. |
| 2 | SupervisionOversight/cuing The participant needs someone to watch over them and make sure they do the task correctly, but they still do all parts of the task themselves. | Ex. The participant is able to get a shower/bath themselves, but needs someone to watch over them to make sure they wash themselves fully and point out what they may have missed. |
| 3 | Limited Assistance Guided maneuvering of limbs, physical guidance without taking weight. The participant needs some physical assistance completing the task, but no weight bearing assistance. | Ex. The participant needs someone to guide their arms and legs into clothes when getting dressed, but does not need any weight bearing support at all. |
| 4 | Extensive Assistance Weight bearing support by 1 person where ptp still performs 50% or more of subtasks. The participant needs some weight bearing support by only one person when completing the task, but are still able to do 50% or more of the task themselves. | Ex. The participant is able to get up from the couch, needs to lean on the caregiver when walking into another room, but then is able to sit back down on their own. |
| 5 | Maximal Assistance The participant needs weight bearing support by 2 or more people OR they need weight bearing support for more than 50% of the task. | Ex. The participant reports that they are capable of bathing the front part of their upper body. However, the participant states that they are unable to lift their arms to complete bathing of their hair and back. In addition, the participant explains that they can not bend to bathe their lower body and need weight bearing support to get into and out of the shower because of balance issues. |
| 6 | Total Dependence The participant has absolutely no involvement in the task. If it weren’t for the caregivers it would not be done. | Ex. The participant is not able to clean themselves up after incontinence episodes. They will sit in soiled garments until someone is able to change her. |
| 8 | Activity did not occur In the past 3 days the task was not done at all. | Ex. The participant is fully incontinent and utilizes diapers only for stooling. Therefore, the participant does not transfer to the toilet. |
Rationale
The rationale is used to define the participant’s capabilities of completing each ADL and IADL as well as calculating how much paid caregiver assistance they need given their capabilities and support system.
This assessment is meant to be Person Centered. Therefore you should ALWAYS review this with the participant and/or responsible parties. NEVER assume information.
Every activity mentioned in the Rationales has to have a descriptive explanation of the care the participant requires, how it is conducted, how often it is needed, and who provides assistance. Gaps in care that may explain an increased request in hours should also be mentioned here.
NOTES:
- For NPO visits, no additional time is allowed to be to listed ADLs/iADLs without supervisor approval.
- If the participant lives with the person who is their paid caregiver, the SC should not be giving any time for shared tasks such as meal preparation, housekeeping and shopping. It is EXPECTED that the person who lives there should be cleaning their own home, preparing shared meals or shopping for their own home without compensation and should be considered informal support.
- Exception to the above rule: The participant is on a diabetic diet and the paid caregiver who lives in the home is not. Therefore, the caregiver is required to prepare separate, special meals for the participant.
NOTE
Answer ALL considerations for each task in the chart below
| Details: | Considerations |
Meal Preparation All the steps of preparing all meals: – planning/choosing what to eat – preparing ingredients/supplies for cooking – Cooking and using appliances – Setting up food/dishes/utensils | HDM – Is the participant receiving HDM? – If so, state how many they receive along with how other meals are prepared throughout the day. – If not, were they offered? Were they accepted or denied? Meal details – How many meals need to be prepared? How long does each meal take to prepare? – Does the participant require a specific diet or modifications to their food? If so, why? Caregiver support – Does formal or informal support live with the participant and share the same meals with the participant? – If not, list the reasons why |
| Ordinary Housework Larger household tasks pertaining to safety and cleanliness: – Dusting/vacuuming – Mopping-Laundry – Cleaning kitchen/bathroom/living areas | Do NOT check off every day and do NOT add additional time. Review board recommends two days weekly for housekeeping. Home details: – What type/size of residence does the participant live in. – Are laundry facilities located on site? – Does the participant live with others? – If the ptp lives with others, note that only the participant’s private areas are to be cleaned by the HHA (i.e. bedroom and bathroom). Otherwise, does the participant live with Informal support and are they able to assist? – If yes, what do they assist with? – If no, list the reasons why not. |
| Managing Finances All aspects of managing finances: – gathering financial document/resources -logging into and navigating online banking -balancing checkbooks/budgeting | – Do NOT check off more than 1 day and do NOT add any additional time – How does a caregiver assist? (i.e. HHA goes to the bank, HHA pays bills online, she reads them to the participant, HHA balances checkbook) |
| Medication Management -Reminding participants to take medications – Ensuring the participant does not choke | – PAS is only allowed to provide verbal reminders. They CANNOT administer medication and/or ensure participant is taking the correct doses. Therefore, no functionality level higher than a 2- Supervision should be selected. – Do NOT add any additional time. – How many medications does the participant take? – Does the ptp have Telecare medication dispensers? If not, was it offered and accepted? If not, why? |
| Phone Use How phone calls are made or received. | – Do NOT add additional time unless there is a legitimate reason such as having 6+ doctors and monthly appointments that need to be scheduled that the HHA assists with. – Do not add more than 0.50 hours. – Does the participant have any cognitive delays or difficulties with communicating? |
| Stairs How a full flight of stairs are managed -Going up and down 12-14 stairs at a time | Home Details – What type of home does the ptp reside in? – Where is their bedroom/bathroom? – Are there stairs inside and/or outside of the home? If so, how many? – If the ptp only has stairs outside of the home, ensure only the days the ptp leaves the home are selected. Ptp Health – Does the ptp have physical limitations caused by diagnoses? If so, describe them. – Does the ptp have any cognitive limitations, such as forgetting that they should not go up and down the stairs alone? If so, describe them. Has a Stair Glide been offered? – What was the ptp’s response to the offer? (i.e. Ptp refused stair glide or accepted it or does not own the home and landlord is not agreeable to stair glide). |
| Shopping How shopping for food and household items is managed: – knowing what items are needed – choosing items and carrying them/putting them in a cart – pushing a cart – paying for items – bagging and carrying items in/out of building/vehicles | -Do not select more than 1 day per week. – How often do they shop? – Does the participant go out shopping with the caregiver or not? – Does the participant live with others? i.e Do they have informal support available to go shopping for them? – Are they receiving HDM and may not need as much groceries? Were they offered and if so list if accepted or declined – Do they have/use grocery delivery services available? |
Transportation How the participant manages using public or private transportation: – Navigating the public transportation system – Paying for fares – Getting in and out of the home and/or vehicles | Forms of transportation – Does the ptp receive a Septa Pass? If so, specify if the HHA goes with the ptp onto transportation and why (If HHA does not go with the ptp, do NOT add time for transportation) – This is NOT about time spent driving the ptp. HHA’s only assist with getting them in and out of the car. Therefore do not add time for length of travel. – Review board recommends only one day weekly for transportation. Reason for travel: – Specify how often the ptp leaves the home and why. – PAS agencies typically do not allow aides to drive in personal vehicles due to liability. The SC should be offering MATP/NMT services and should document the response to the offer. |
| Bathing How a full bath/shower is completed: – getting in and out of the tub/shower – Setting up assistive devices for bathing/showering – Washing and drying each part of the body (except hair and back) – Bed bathing the participant along with set up to do so | Review Board recommends bathing only three times weekly. – If the ptp suffers from skin conditions or pressure ulcers, make sure it is defined in the rationale and in Section 53 of the InterRai. Explain why multiple baths might be needed for that participant throughout the day. Home Mods/DME – What DME/Home mods does the ptp have already? List the items – If none, were they offered? (i.e. Home Mods, shower chairs, grab bars). Were they accepted or denied? – If accepted, does the ptp own the home? – If denied, explain why. Caregiver Support – How does the caregiver assist the ptp? – How much time is spent to complete the bath/shower? |
| Personal Hygiene Completing all personal hygiene tasks: – Combing/brushing hair – Shaving- brushing teeth – applying make-up – washing/drying face and hands -lotion/deodorant application | – Do NOT duplicate justification from bathing. – Does the HHA provide set up or hands-on-help? – What can the ptp do independently? -What does the informal assist with? |
| Dressing Upper Body How they dress/undress the upper body: – choosing appropriate clothing – putting on bra -pulling clothes over their head -putting arms through the sleeves -Fastening buttons/zippers | – Why does the ptp need assistance? – What can the participant do independently and what does the HHA do to assist? – Is informal support available to assist? |
| Dressing Lower Body How they dress/undress the lower body: – choosing appropriate clothing – putting on underwear – stepping into clothes and pulling them up to the waist (if applicable) – Fastening buttons/zippers | – Why does the ptp need assistance? – What can the participant do independently and what does the HHA do to assist? – Does the participant have buttons/zippers – Is informal support available to assist? |
| Walking | -The functionality level selected in walking must match locomotion. |
| Locomotion How the participant receives assistance with assistive devices when walking or with a wheelchair: -Retrieving/setting up assistive devices -Reminders about using assistive devices -Being pushed in a wheelchair | – Do NOT duplicate information from the walking section – What assistive devices does the ptp use? – What assistance is provided for use of canes/walkers/wheelchairs? (i.e. reminders to use cane, needs walker brought to them, needs to be pushed once in their wheelchair) – What is the participant able to do on their own? -Should the next level of device be offered (ie. if ptp needs maximum help to move with the walker and is still struggling, have we offered a wheelchair or recommended they talk to PCP about one?) – Does the participant require supervision or physical assistance while walking? If so, why? – Does the participant have any assistive devices? (ie. walker, cane, wheelchair) – If so, describe them – If not, were they offered? – How many trips to the bathroom per day does the participant require assistance? |
Transfer Toilet Assistance getting on and off of a toilet or commode: -GOING TO AND FROM THE BATHROOM is NOT included | – Do NOT include time walking to the bathroom – Who assists the participant? – How many times a day does the ptp go to the bathroom on average? – Does the participant have any Home mods, DMEs, or SMEs? (i.e grab bars, raised toilet seat, commodes, urinals)- If yes, state them- If no, were Home Mods/DME/SME offered? Did the participant accept or deny? – Does the ptp have any incontinence diagnoses or take any medications that affect balance during transfers? |
| Toilet Use -Assistance using the toilet and/or commode/urinal or management of incontinence supplies -wiping/cleaning themselves -changing pads/incontinence supplies -managing ostomy/catheters -re-adjusting clothes | – Do NOT include time walking to the bathroom – Does the participant use the toilet, incontinence supplies, or both? Describe why the participant uses any devices – How many times a day does the ptp go to the bathroom on average? -What assistive devices have we offered (ie. commode, urinal, raised toilet seat, incontinence supplies) and were they accepted or declined. – If the participant is fully incontinent and only uses diapers for stooling, there should be NO time in toilet transfer. |
| Bed Mobility -Moving/changing positions in bed – moving to and from lying down to sitting up – moving from side to side in the bed/rolling over – changing position in the bed | – What assistance is provided? (i.e. HHA provides assistance by handing cane and helping to transfer in and out of bed). – How many times per day OR how often does the ptp require assistance (i.e. helping twice per day or repositioning every 2 hours to prevent bed sores) – Was DME offered? (i.e. Hoyer Lift?) |
| Eating -How the participant eats/drinks? – includes tube feeding and other means of eatingbeing fed and supervision to prevent choking | – Do NOT include time for modifying food. That is for Meal Prep – Does the participant need assistance to set up utensils, dishes, napkins, cups, etc? – Does the participant need assistance being fed or given reminders to eat due to diagnoses. – Does the participant eat orally or through tube feeding? |
Related Post
