
Follow Up
Categories :
Clinical/Hospitalization
Transitional Care planning-Clinical/Hospitalization
Used to document interaction regarding participant discharge from the hospital
- Session Requires:
- Appropriate answers to all required questions
Example:

Process:
- When a Service Coordinator becomes aware that a participant has been hospitalized, then the SC begins making calls to the participant and Hospital to discuss discharge planning
- Once the SC has made successful contact to discuss the discharge plan, then Transitional Care Planning Session is completed
Documentation:
- Transitional Care planning
- Note category- select whether the successful contact to discuss discharge was an Incoming or Outbound call
- Contact name- First and last name of the person the SC spoke with is listed here
- Call recipient type- select the appropriate option
- If other is selected, additional required question must be answered
- Name of the hospital where participant is currently admitted- NO abbreviations, list hospital’s full name (ie. Jefferson Health-Abington)
- Name and contact information of the Social Worker- First and Last name required, as well as phone number to reach them at
- Date participant was admitted to the hospital
- Potential Date of discharge- you must enter a date
- Address to which participant is being discharged
- Does the participant have any additional services/medications/etc being recommended at discharge?
- This includes all types of services that are not already in place as well as increases recommended to current services
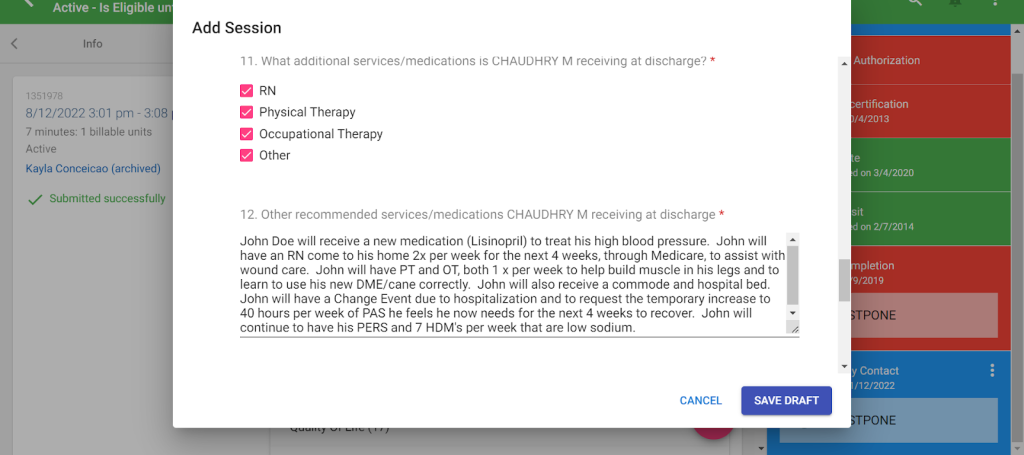
- What additional services/medications is the participant receiving at discharge?
- Select appropriate options, more than one can be selected
- “Other” must be selected and all new services must be entered
- Who will be assisting the participant with attaining services/medications?
- Select the appropriate option
- If “other” is selected you must provide additional information on who else will be assisting

- Additional comments regarding the discharge
- Enter any other relevant information that was discussed during the discharge planning conversation
Non clinical/Rehab
Transitional Care planning- Non-Clinical/Rehab
Used to document interaction regarding participant discharge from the Nursing Facility/Rehab
- Session Requires:
- Appropriate answers to all required questions
Example:

Process:
- When an Service Coordinator becomes aware that a participant has been admitted to a Nursing Facility/Rehab, then the SC begins making calls to the participant and facility to discuss discharge planning
- Once the SC has made successful contact to discuss the discharge plan, then Transitional Care Planning Session is completed
Documentation:
- Transitional Care planning
- Does the participant want to transition from NF?
- If the participant does not want to transition from the Nursing Facility then additional details on why are provided
- Does the participant want to transition from NF?
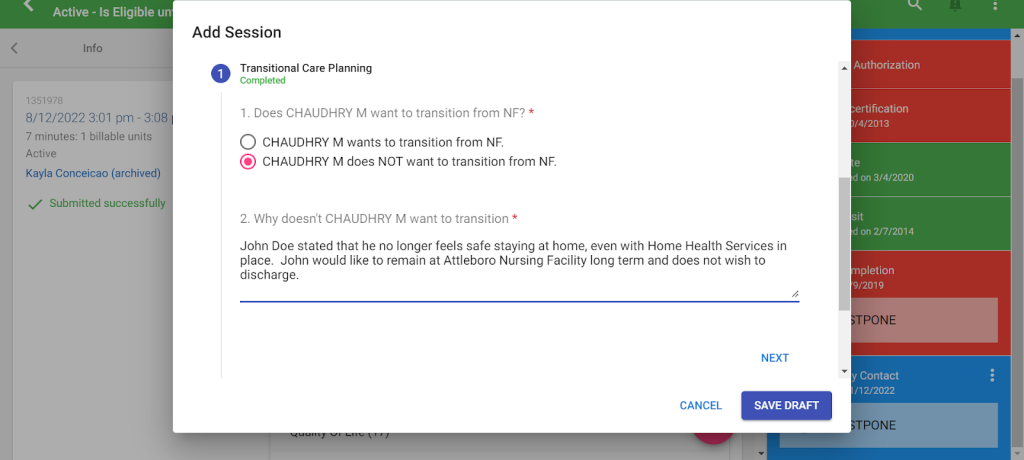
- Transition Details
- If the participant does not want to transition then this section is not completed.
- If the participant wishes to transition then the following must be answered.
- Does the participant have housing to transition to?
- Are home modifications will be needed?
- Does the participant have major medical concerns?
- What major medical concerns does the participant have?
- Does the participant have a discharge date?
- Discharge date?
- What skilled services is the participant receiving at discharge?
- Select the appropriate option(s), more than one can be selected
- This includes all types of services that are not already in place as well as increases recommended to current services
- Other skilled services the participant is receiving at discharge?
- List specific details on all services the participant will have at time of discharge from the facility
- Does the participant have a POA/Guardian?
- First and last name of POA/Guardian
- If you list a POA, you must then attain a copy of POA or Guardianship paperwork and upload into Function portal
- Has POA/Guardian been called to discuss discharge?
- POA/Guardians comment on transition
- Reason POA/Guardian has not been called
- First and last name of Social worker
- Phone number of social worker
- Has the social worker been called to discuss discharge?
- Social worker comment on transition
- Reason social worker has not been called
- Does the participant have a Family/Caregivers
- First and last name of Family/Caregivers
- Phone number of Family/Caregivers
- Has Family/Caregivers been called to discuss discharge?
- Family/Caregivers comment on transition
- Reason Family/Caregivers has not been called
- Other
- Additional comments concerning the transition (ie. new medications, services, etc being recommended or prescribed)
- Provide any other relevant information regarding discharge planning that is not already documented in the session
- Does an email need to be sent to the Nursing Home Transition (NHT) team?
- If the participant has been in the Nursing Facility for short term care, then select that NHT email is not needed
- If the participant has been in the Nursing Facility for long term care and requires the assistance of the Nursing home transition team to return to the community, then select that the NHT email is needed
- If you are unsure of the appropriate selection, discuss with your Supervisor
- Additional comments concerning the transition (ie. new medications, services, etc being recommended or prescribed)
Related Post
