
Change Event
Categories :
Change Event Session
Used to document Change in Condition visits.
- Session Requires:
- Appropriate answers to all required questions
- Corresponding sessions:
- InterRAI session
- HEDIS session
- HRA/DSNP
- PCSP session
- Required Forms session
Example:
Process
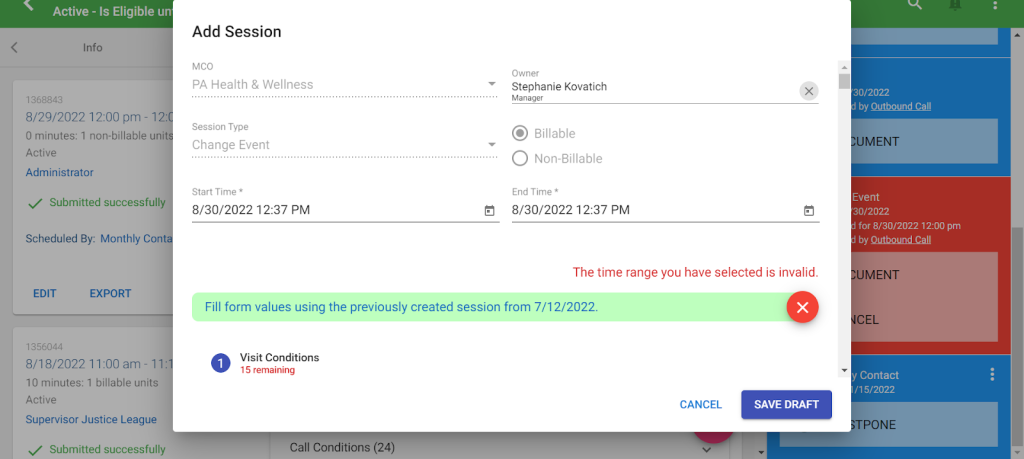
- Once Change Event visit is scheduled in Function Portal, there will be an alert on the right side of the screen to Document the Change Event Session
Example:

Documentation
- Visit Conditions
- Which of the following occurred? – Select what change(s) occurred for the participant, necessitating the visit.
- Select one, or BOTH, options based on the participant’s reported changes
- Visit Type – How are you contacting the participant
- Select the appropriate answer.
- If the visit was Face to Face, answer:
- Who was present during the visit?
- Covid 19 Screening session will need to be done for all face to face visits
- If the visit was Face to Face, answer:
- Select the appropriate answer.
- Which of the following occurred? – Select what change(s) occurred for the participant, necessitating the visit.
This information MUST match the answer provided in the PCSP in Function Portal
- Did the member accept or decline the Virtual Visit? – select if the member accepted virtual visit or why they declined
- If the visit was done virtually, select Member Accepted
- If the virtual visit was declined for other reasons answer:
- Reason for declining Virtual Visit
- Was the Legal Representative invited to participate? – If the participant has a legal representative, did the SC or the participant try to involve the participant’s Legally Authorized Representative?
- Answer is based on if your participant has a rep and invited them or not
- Based on your answer you may need to answer the following:
- Did the Legal Representative participate in the contact?
- Did the member request that the legal representative not participate?
- Where did the visit take place? – This should correspond with the Visit Type answered above
- Where does the participant currently reside? – Coordinator should be confirming the client’s address and type of residence, then choose the appropriate answer.
- If the answer was “Home (with a caregiver)” then the coordinator needs the following information about the caregiver.
- Caregiver name
- Caregiver relationship to participant
- Does the caregiver live with member?
- Does the caregiver provide natural support? – meaning does the caregiver provide informal/unpaid support?
- Is the caregiver paid?– meaning does the caregiver provide formal/paid support?
- If the answer was “Other” then the coordinator needs to state what the Other residential location is
- If the answer was: “AFCH, ALF, Hospice, or Nursing Home” the the caregiver must state what the Residential location facility name
- If the answer was “Home (with a caregiver)” then the coordinator needs the following information about the caregiver.
- Information provided by – Meaning who did the coordinator speak with during the call.
- If the answer involved “Other” then the SC needs to state who this other person was and why they spoke to them.
- Has the participant expressed the desire to move from an institutional setting to the community? – participants have to be currently residing in an institution, which most of our clients do not.
- Answer is most likely – Participant has NOT expressed desire…
- If the answer was “Participant has expressed desire …” the coordinator needs to state the current transition status
- Did the participant’s demographics change? – Has any of the information about the participant changed?
- If there was a change, then the coordinator must state what the changes are.
- Member materials provided – Describe any resources, materials, or referrals that were given to the participant
- Was the member referred to Nurtur?
- Was the member referred to Disease Management?
- Was the member referred to Behavioral Health?
- Did the CC review the Member Handbook with the enrollee/authorized representative?
- If the Handbook was NOT reviewed, explain why.
- Which Advanced Directives does the enrollee have? – select the advanced directives the participant has or None, but importance was discussed
- If the answer was “Other Advanced Directives” explain what other advanced directives the ptp has.
This information should match the answers provided in the PCSP (Life Planning section)
- Change Event
- Questions here will only generate based on the selection(s) to which of the following occurred? asked in the previous section
- Describe what prompted the participant’s change in Health Condition – detailed description about the participant’s health changes and/or incidents that occurred to cause changes in health condition.
- If the enrollee is not capable of making decisions …? – select if referral or other resources were provided to the participant regarding inability to make their own decisions and lack of legal representative.
- Was this a significant change that required the HRA to be updated? – HRA is the Health Risk Assessment or DSNP (Dual-eligible Special Needs Plan)
- What changes are needed to the Plan of Care? – select all the changes that occurred within the PCSP, compared to previous, or select “No changes”
- If changes were selected, describe the details of the changes
- If enrollee/authorized rep was unable or refused to sign… explain why – If the PCSP could not be signed while in person, explain why. If the PCSP could not be signed because the visit was not Face to Face, state that.
- Medical Conditions
- What changes to health did the participant report? – select if the participant feels their health has improved, declined, or remained the same
- Were there any changes to the participant’s medications or diagnoses?
- Since last visit, has the participant visited any of these? – select any of the listed appointments that the participant has attended since the last visit was done. If “No visits” occurred, select that.
- If any visits occurred, provide details about the type of visit, why it was completed, and approximately when it occurred.
- Does the participant have any special needs?
- If the participant has special needs the coordinator must state what the special needs are in Special needs details
- Goals
- What is the participant’s status of goals …? – select which option best applies to the discussion of goals made with the participant.
- Describe what was discussed about the goals in Goal status comments
- What is the participant’s selection for Participant Directed Option? – does the participant have Tempus as their PAS provider? If so, select “Enrollee elected PDO”. If not, select “Enrollee does not wish to elect PDO at this time”
- If “Enrollee elected PDO” is selected, describe what the participant is doing with their PDO (such as who their DCW and back up plan is)
- What is the participant’s status of goals …? – select which option best applies to the discussion of goals made with the participant.
- Informal Support
- Does the participant receive informal support for Activities of Daily Living?
- If “participant receives informal support” answer the following:
- Supporter name
- Relationship to the participant
- Minimum hours informal support may provide
- Maximum hours informal support may provide
- If “participant receives informal support” answer the following:
- Does the participant receive informal support for Activities of Daily Living?
- Observations of Participant and Environment
- Describe Participant’s environment and any concerns
- If visit is Face to face describe your observations
- If visit is over the phone, have the participant describe their environment.
- Describe Participant’s environment and any concerns
This information should match the answers provided in the InterRAI and PCSP
- How was the participant dressed? Were they clean? (nails, hair, clothing)
- If visit is Face to face describe your observations
- If visit is over the phone, state you were unable to observe
- What was the participant wearing? – state which common assistive devices the participant wears
- Select if the participant was wearing dentures, hearing aids, and/or glasses.
- How were they moving around? – How the participant ambulated or regularly ambulates
- Select if the participant moves with or without assistive devices, or if they are bed bound
This information should match the answers provided in the InterRAI
- Participant Story – Basic health information about the participant
- You can cut and paste the story put into the PCSP (Page 2) for Daily Routine
- This story should include the following information”
- Name
- Age
- Gender and Race
- Diagnoses
- Number of Medications
- Living Accommodations
- Formal/Informal Support
- ADLs and IADLs they require assistance with
- This story should include the following information”
- You can cut and paste the story put into the PCSP (Page 2) for Daily Routine
- Observations of Participant’s Mood/Behavior
- Describe the enrollee’s appearance, mood and behavior … – describe anything you can about the participant, even if the visit is not Face to Face.
- Activities of Daily Living
- Coordinators must state how much assistance the participant needs with the following ADLs
- Bathing, Dressing, Grooming, Eating, Transferring, Toileting, and Bladder Management
- Does the participant receive informal support for activities of daily living?
- If the participant has informal support then the coordinator needs to state the name, relationship and average minimum and maximum hours of support they provide each day.
- Does the participant have unmet needs for daily living? – Does the participant need any services or devices?
- If the participant has unmet needs then the coordinator needs to put in what these unmet needs are in Describe
- Does the participant use assistive devices/durable medical equipment for activities of daily living?
- If the participant feels they would benefit from assistive devices/durable medical equipment then the coordinator needs to state details in Describe
- Coordinators must state how much assistance the participant needs with the following ADLs
All of this information should match the answers provided in InterRAI
- Satisfaction
- Is the participant satisfied with services and/or providers reflected on their plan of care?
- If the participant is not satisfied with any of their services, the coordinator needs to state what they are doing to address the dissatisfaction
- Is the participant receiving adult daycare services? – A common service that participants may receive
- If the participant receives ADC services then coordinator must state how satisfied they are with the service
- If the participant is dissatisfied with the service, coordinator needs to state the reason they are dissatisfied
- If the participant receives ADC services then coordinator must state how satisfied they are with the service
- Is the participant receiving care coordination services? – All participants receive care coordination so the answer should always be – Participant is receiving care coordination services
- How satisfied is the participant with their Care Coordinator? – Coordinator must state the participant’s satisfaction with Amcord Care.
- If the participant is dissatisfied with the service, coordinator needs to state the reason they are dissatisfied
- How satisfied is the participant with their Care Coordinator? – Coordinator must state the participant’s satisfaction with Amcord Care.
- Does the participant have a health plan? – All participants have a health plan, it is PA Health & Wellness, therefore the answer should always be – Participant has a Health Plan
- How satisfied is the participant with their Health Plan? – Coordinator must state the particpant’s satisfaction with PHW.
- If the participant is dissatisfied with the service, coordinator needs to state the reason they are dissatisfied
- How satisfied is the participant with their Health Plan? – Coordinator must state the particpant’s satisfaction with PHW.
- Does the participant have a personal care attendant? – Most participants have a personal care attendant, it is PAS, therefore the answer is likely Participant has a personal care attendant
- If the participant receives PAS, then coordinator must state how satisfied they are with the service
- If the participant is dissatisfied with the service, coordinator needs to state the reason they are dissatisfied
- If the participant receives PAS, then coordinator must state how satisfied they are with the service
- Does the participant have a transportation provider? – A common service that participants may receive
- If the participant receives transportation services then coordinator must state how satisfied they are with the service
- If the participant is dissatisfied with the service, coordinator needs to state the reason they are dissatisfied
- If the participant receives transportation services then coordinator must state how satisfied they are with the service
- Is the participant satisfied with services and/or providers reflected on their plan of care?
- Quality of Life
- Coordinators must go through the following and answer honestly
- Has the participant received a pneumovax vaccine since turning 65?
- Has the participant received a flu vaccine in the last 12 months?
- Does the participant have issues with bladder control?
- If the participant has issues with bladder control, then SC must answer: bladder control issue frequency
- Has the participant had a UTI in the past 3 months?
- Does the participant have issues with bowel control?
- If the participant has issues with bowel control, then SC must answer: bowel control issue frequency
- Does the participant have any skin breakdown?
- If the participant has skin breakdown, then SC must answer what type of breakdown there is (bruising, incision, tears, or wounds)
- Has the participant had any falls since the last contact?
- If the participant has had a fall, SC must answer the following:
- How many falls has the participant experiences in the last 3 months
- Did the falls result in an injury?
- If the fall resulted in an injury, then SC must answer Fall injury treatment
- If the participant has had a fall, SC must answer the following:
- Is the participant able to do things they enjoy outside of their home and with whom they want?
- Is the participant able to make decisions about their daily routine?
- Does the participant feel safe in their home/where they live?
- Does the participant have a paid or volunteer job in the community?
- Does the participant like where they are living?
- Does the participant see or talk to friends and family with whom they do not live?
- Coordinators must go through the following and answer honestly
- Resolution
- Did the member or Legal Rep, if applicable, sign the PCSP?
This answer should match the answer provided in all documentation for this visit
- Did the external Service Coordinator sign the PCSP? – Answer should always be YES (you are the external service coordinator)
- Was there a change to the services authorized? – Are there any changes to the services being requested during this visit?
- If a change is requested, answer the following:
- Was there an increase or decrease in the amount of services?
- Did the member request the increase/decrease?
- What was the reason for the increase?
- If a change is requested, answer the following:
Related Post
