
Signatures and Releases of Information
The Releases are a collection of authorization, consent, and demographic forms required for each Comprehensive Needs Assessment Visit.
Information in these forms MUST be consistent with the information presented in all other documents of the visit (I.e. InterRAI, Visit session in FP, HRA/DSNP, PCSP)
Signing the Releases
To sign the releases, during any visit, look on the right hand side of the Function Portal screen, for the alert called “Required Forms”. Select the “Document” button to open the session.
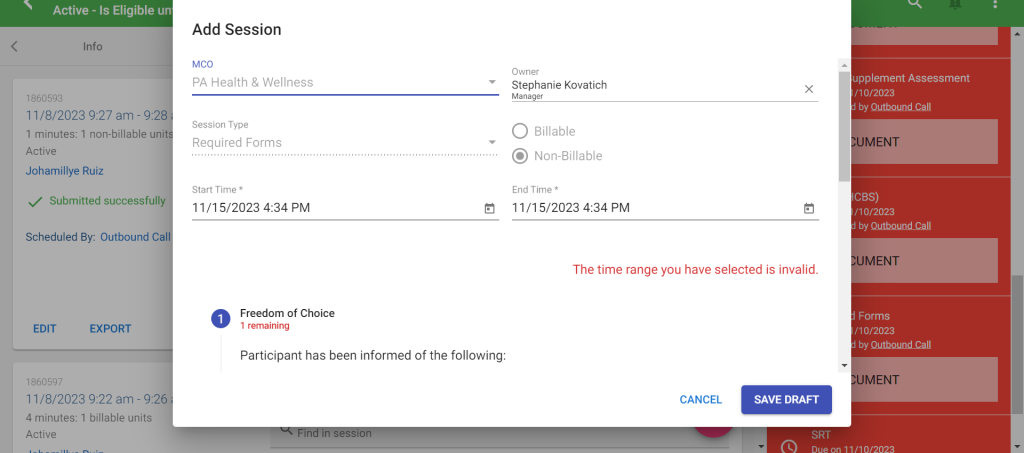
Required Forms Session
This session includes the HIPAA Authorization to disclose form and the Freedom of Choice form. Both are required to be signed by the SC and the participant/POA. If the POA is signing, there is an option in this session to upload the POA documents that are required in order for anyone saying they are a POA to sign on behalf of a participant.
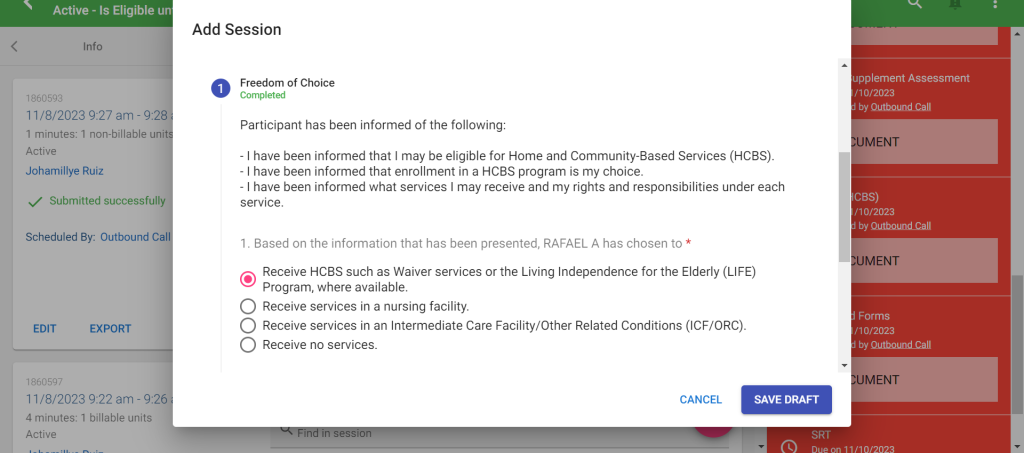
Freedom of Choice form will require the SC to review certain information with the participant/POA and to make a selection of the participant’s choice to receive services.
Example: The participant has selected to continue to receive Waiver services in their home
HIPAA Authorization to disclose form will require the SC to discuss with the participant/POA what information of the participant’s they would like shared and who they would like it shared with. The SC must collect all of the contact information in the session, in order for this form to be considered filled out correctly. There are 8 spots for additional recipients/contacts to be added and this should include anyone the participant chooses.
Example: Participant is fine with all information being shared with their daughter/Betty Smith.

Find previously uploaded documents as Annual_Contact_Packet or Orientation_Packet in Function Portal, in the “Attachments” tab.
Related Post
