
Have a Question?
HEDIS Assessment
Healthcare Effective Data and Information Set
An assessment to review the participant’s self efficacy and loneliness in their day to day life.
Completed for every Comprehensive Needs Assessment visit (i.e. NPO visits, Annuals, and Change Events)
The assessment will calculate a level of efficacy and loneliness for the participant
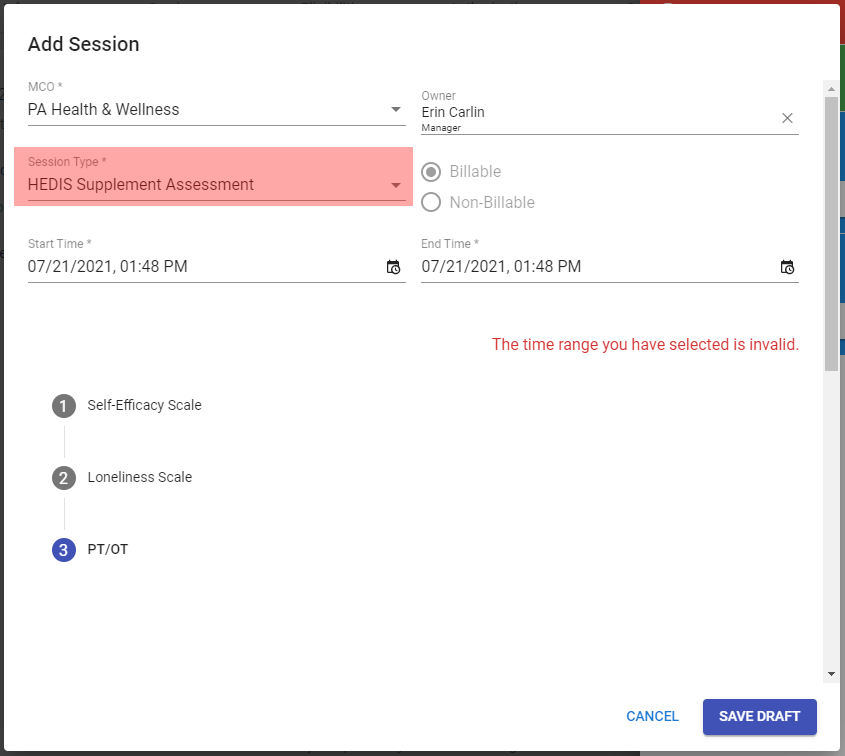
- Self Efficacy Scale
This section MUST be answered by the participant, NOT the POA, legal rep, or responsible party.
- Is the participant cognitively intact and able to provide efficacy information?
- If the participant is cognitively able to provide answers, select “Participant is cognitively intact and able to provide efficacy information”
- If the participant is is too cognitively impaired to answer these questions, select “There is documentation to support that the participant is too cognitively impaired
The following questions of this section must be answered by the participant. Have them give an answer from 1-10
“1” represents “not at all confident” and “10” represents “totally confident”
- How confident do you feel that you can keep the fatigue caused by your disease from interfering with the things you want to do?
- How confident do you feel that you can keep the physical discomfort or pain of your disease from interfering with the things you want to do?
- How confident do you feel that you can keep any other symptoms or health problems you have from interfering with the things you want to do?
- How confident do you feel that you can keep the emotional distress caused by your disease from interfering with the things you want to do?
- How confident do you feel that you can do the different tasks and activities needed to manage your health condition so as to reduce your need to see a doctor?
- How confident do you feel that you can do things other than just taking medication to reduce how much your illness affects your everyday life?
After answering all questions an average efficacy score will be generated
- Loneliness scale
This section MUST be answered by the participant, NOT the POA, legal rep, or responsible party.
- Is the participant cognitively intact and able to provide efficacy information?
- If the participant is cognitively able to provide answers, select “Participant is cognitively intact and able to provide efficacy information”
- If the participant is is too cognitively impaired to answer these questions, select “There is documentation to support that the participant is too cognitively impaired
- During the past month, the participant has often been bothered by feeling lonely?
- If the participant has often felt lonely, they will need to answer the remaining questions
- If the participant has NOT often felt lonely then they will not need to answer the remaining questions
- How often do you feel that you lack companionship?
- How often do you feel left out?
- How often do you feel isolated from others?
After answering all questions the sum of responses will be generated
- PT/OT
This section may be answered by the Participant, POA, legal rep, or responsible party
- Does the participant need Physical Therapy or Occupational therapy?
- If the participant states they need PT or OT, you will need to answer Is the participant receiving PT/OT?
- What home health services does the participant receive?
- Select the services that the participant receives
- Home Health Aid – this is NOT PAS (it is typically paid by Medicare)
- Nurse Visit – Wound care nurse, RN, LPN
- Other – includes Medicaid services such as: PAS, PERS, HDM, NMT
- Select the services that the participant receives